
Conceptual Frameworks for Classifying Pharyngeal Motor Disorders
Physiological Measures
If P-HRM-I detectable phenomena and objective metrics are to reliably inform the design of a classification system for characterising pharyngeal motor disorders, they must be able to distinguish disorders of upper esophageal sphincter (UES) outflow (UES Dysfunction) and/or disorders of pharyngeal propulsion and clearance (Pharyngeal Dysfunction).
Fortunately, the expert guidance on P-HRM-I analyses of oropharyngeal swallowing already includes recommendations for how to derive the key physiological measures that define these dysfunctions. These recommendations can be found in the original Working Group publication and are illustrated in the Figure below.
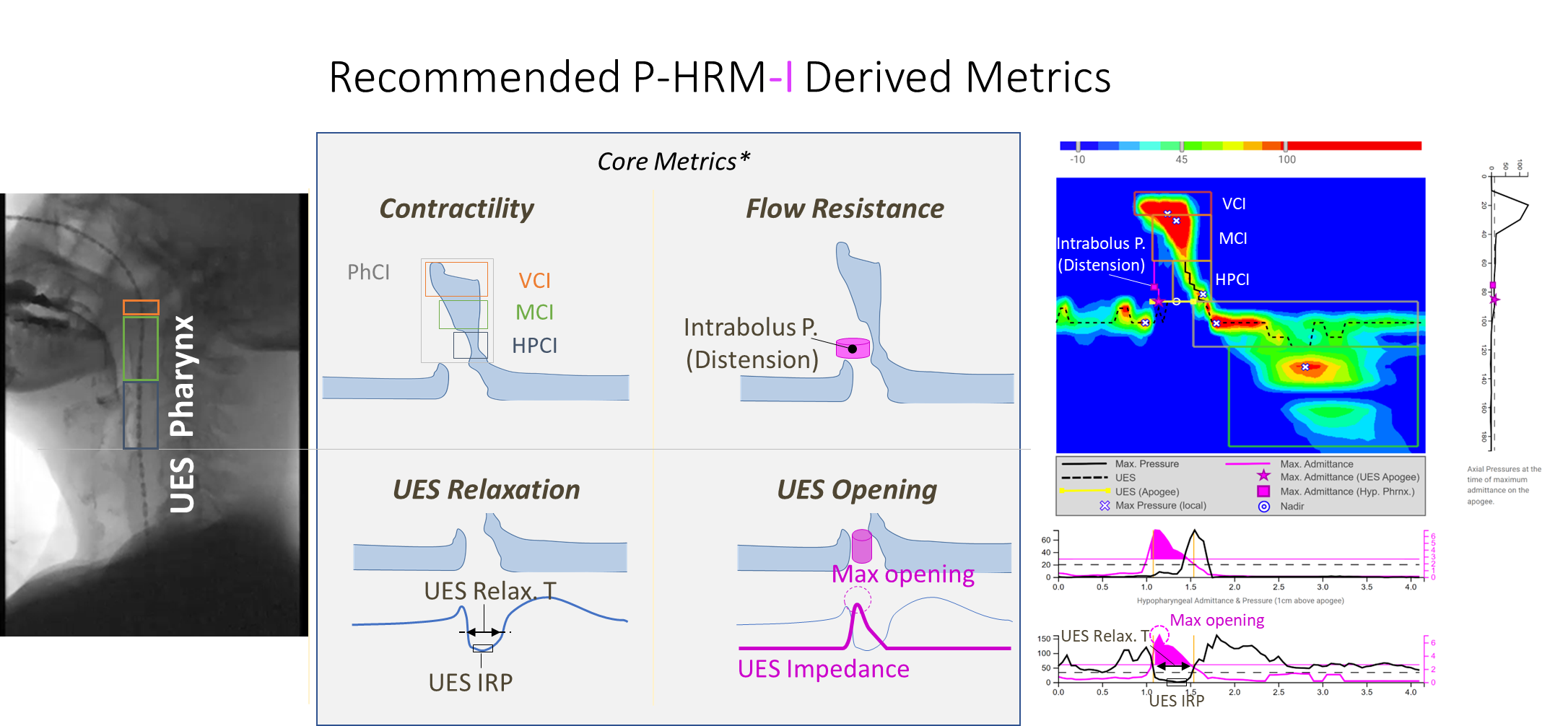
UES Dysfunction
The objective measures of upper sphincter function include UES integrated relaxation pressure (UES IRP), reflecting the lowest pressures during UES relaxation, and are considered a highly useful metric for indicating UES dysfunction based on a high UES IRP value. UES IRP is, however, a complex metric influenced by both contraction and distension pressures; identification of a UES relaxation disorder could therefore also be supported by, for example, evidence of short UES relaxation time, high intrabolus distension pressure (IBP) and/or low UES maximum admittance (UES Max.Adm). Different pharyngeal pressurization patterns may also point to UES dysfunction.
Pharyngeal Dysfunction
A pharyngeal propulsion or clearance disorder is characterised by direct measurement of the pressure generated by the pharyngeal contractile sequence, from the velopharynx through to the hypopharynx. The objective measures of pharyngeal contractility can indicate whether contractility is impaired globally, across the whole pharyngeal sequence, or within specific regional sub-components of the sequence.
Conceptual Framework Underpinned by Swallow Function Metrics
The ability to derive the physiological swallowing data above has already proven useful for characterizing the physiological and potential rehabilitative effects of swallowing exercise, sensory stimulation, fluid viscosity modification, novel surgical interventions, such as cricopharyngeal POEM, and neuro-stimulation paradigms, such as pharyngeal electrical stimulation. Direct P-HRM-I assessment of swallowing physiology can complement routine clinical and instrumental swallowing assessments, adding understanding of dysphagia pathophysiology, and may help to guide patient management.
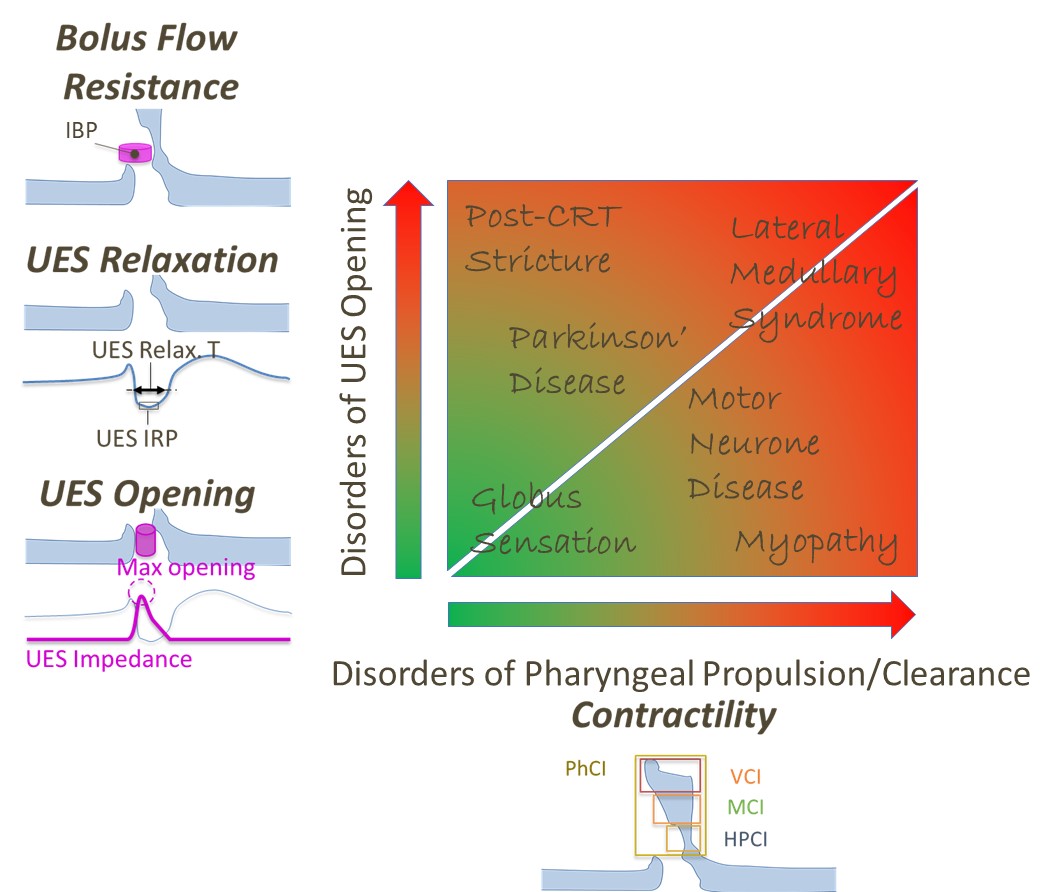
The capacity to group findings into broad categories of abnormality is also valuable for clinical translation. The simplest such grouping distinguishes two categories. While it is convenient to treat UES and pharyngeal dysfunctions separately, they are, of course, interrelated and may both be present, to varying degrees, in different patients undergoing P-HRM-I studies, as illustrated in the Figure below.
For clinical utility, we need to understand which P-HRM-I measures differentiate pathological swallowing in patients reporting symptoms of dysphagia from normal swallowing in healthy people.
Before proceeding further, it is recommended that you read the paper, 'Using high resolution manometry impedance to diagnose upper esophageal sphincter and pharyngeal motor disorders' (found below), which presents data from a large research audit of patients undergoing P-HRM-I and analyzed using Swallow Gateway. Additional data drawn from this published dataset will be discussed in the pages that follow.